
Referred pain
Updated July 2009
If you woke up with a pain in your shoulder, you'd probably think something was wrong with your shoulder, right? Maybe you slept on it the wrong way, maybe you're a weekend warrior who threw the football a few too many times. In most cases, your hunch is probably right. Pain in the shoulder usually indicates an injury or disease that affects a structure in your shoulder, such as, say, your subacromial bursa or a rotator cuff tendon. Makes sense, doesn't it?
But you might be way off. Sometimes the brain gets confused, making you think that one part of the body hurts, when in fact another part of the body, far removed from the pain, is the real source of trouble. This curious (and clinically important) phenomenon is known as referred pain. For example, it's unlikely but possible that your shoulder pain is a sign of something insidious happening in your liver, gall bladder, stomach, spleen, lungs, or pericardial sac (the connective tissue bag containing the heart). Strange, isn't it? Conditions as diverse as liver abscesses, gallstones, gastric ulcers, splenic rupture, pneumonia, and pericarditis can all cause shoulder pain. How is that possible?
Neuroscientists still don't know precisely which anatomical connections are responsible for referred pain, but the prevailing explanation seems to work pretty well. In a nutshell, referred pain happens when nerve fibers from regions of high sensory input (such as the skin) and nerve fibers from regions of normally low sensory input (such as the internal organs) happen to converge on the same levels of the spinal cord. The best known example is pain experienced during a heart attack. Nerves from damaged heart tissue convey pain signals to spinal cord levels T1-T4 on the left side, which happen to be the same levels that receive sensation from the left side of the chest and part of the left arm. The brain isn't used to receiving such strong signals from the heart, so it interprets them as pain in the chest and left arm.
So what about that shoulder pain? All of organs listed above bump up against the diaphragm, the thin, dome-shaped muscle that moves up and down with every breath. The diaphragm is innervated by two phrenic nerves (left and right), which emerge from spinal cord levels C3, C4, and C5 (medical students remember these spinal cord levels using the mnemonic, "C3, 4, 5 keeps the diaphragm alive"). The phrenic nerves carry both motor and sensory impulses, so they make the diaphragm move and they convey sensation from the diaphragm to the central nervous system.
Most of the time there isn't any sensation to convey from the diaphragm, at least at the conscious level. But if a nearby organ gets sick, it may irritate the diaphragm, and the sensory fibers of one of the phrenic nerves are flooded with pain signals that travel to the spinal cord (at C3-C5). It turns out that C3 and C4 don't just keep the diaphragm alive; neurons at these two spinal cord levels also receive sensation from the shoulders (via the supraclavicular nerves). So when pain neurons at C3 and C4 sound the alarm, the brain assumes (quite reasonably) that the shoulder is to blame. Usually that's a good assumption, but sometimes it's wrong.
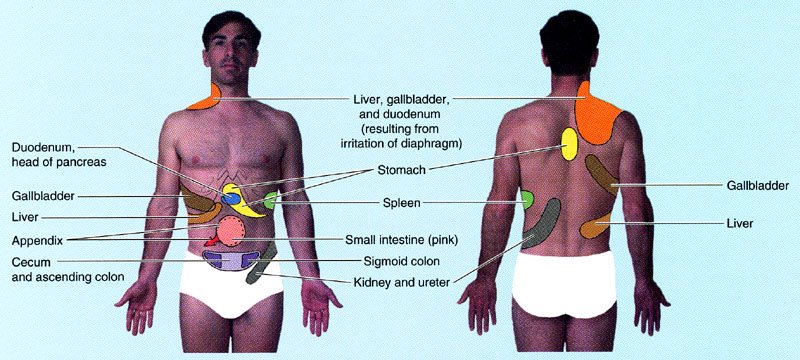 Illustration showing sites of referred pain from abdominal organs. From Moore and Dalley's Clinically Oriented Anatomy. Please note that I added the "tighty whities" with Photoshop (hey, this is a family friendly site).
Illustration showing sites of referred pain from abdominal organs. From Moore and Dalley's Clinically Oriented Anatomy. Please note that I added the "tighty whities" with Photoshop (hey, this is a family friendly site).Another example that seems bizarre until you know the anatomy is disease in the stomach causing pain between the shoulder blades. A classmate told me that one of her college professors complained to his doctor about pain in his upper back that wouldn't go away. It turns out that the professor had gastric cancer, a relatively aggressive and often incurable disease unless it's caught early. Unfortunately it wasn't caught early enough and it ended up taking his life. Maybe the outcome would have been different if the doctor had remembered that some of the nerve fibers to the stomach (specifically, visceral afferents that travel in the greater splanchnic nerve) convey pain signals to the same spinal cord levels (especially T5 and T6) that receive pain signals from the skin between the shoulder blades. This variety of referred pain is rare, but it happens often enough to be mentioned in anatomy textbooks.
Not all cases of referred pain are easy to find in textbooks. Take the appendix, for instance. That wormy little appendage of the colon is usually located in the right lower quadrant of the belly, nowhere near the diaphragm. Typically people with appendicitis feel diffuse pain or discomfort around the belly button, or sharp pain in the right lower quadrant if the appendix is getting ready to burst. But occasionally the pain refers to the right shoulder. Why? Note that I said the appendix is usually located in right lower quadrant. Sometimes, early in embryological development, the colon doesn't rotate as much as it should, and the appendix ends up in the right upper quadrant (or even on the left side of the belly). That malrotation isn't necessarily a problem for the patient until the appendix becomes swollen with infection, irritating both the diaphragm and the doctor who is trying to make a diagnosis!
So if your shoulder happens to hurt right now, should you be worrying about something bad in your belly? Probably not. The most common causes of shoulder pain are, by far, musculoskeletal problems like osteoarthritis, adhesive capsulitis, and rotator cuff tendinitis. Often, with the help of taking it easy and a few rounds of ibuprofen, the pain goes away on its own. But if you're still concerned, make an appointment with your family physician. Red flags include more ominous symptoms like fever, unexplained weight loss, and pain in the left shoulder or scapular area that gets worse with exertion.
Your doctor will want to know all about the pain. Was there a specific injury or did the pain come on slowly? Does the pain occur without movement of the shoulder? Can you make it worse with specific movements? Are there any other symptoms or chronic medical problems? The answers to these questions, along with a physical exam and appropriate imaging studies, will provide the information your doctor needs to understand the problem and create a treatment plan. The odds are good that the problem is relatively common and treatable. But if your doctor seems stumped, it wouldn't hurt to ask, "Is there any chance this could be referred pain?"
posted by Brad @ 4:45 AM
338 comments
![]()
![]()



338 Comments:
Now if you could just figure out why my legs hurt from the sores in my mouth!
Great Post Doc!
This is brilliant !
I`ve bookmarked this page for reference.
Thanks for the info !
Excellent post! This is one of those instances that clinicians often forget about when diagnosing problems. Horses for example can exhibit back and forelimb soreness and tenderness when suffering from colic (bowel obstruction) or even dental abscesses.
Great post - Very informative. Thank you!
In fact, I may link to you from my blog
Fibromyalgia Research Blog
http://glutenfreebay.blogspot.com
Interesting observations, madveterinarian. They remind me of another example of referred pain that I can't explain: jaw pain during a heart attack.
very well written!
Hey, Finally added you to blog ring. Sorry for the delay ;)
Blogs of Medical Students
Hi brad, I'm a medical student in China and this term we learned the course of Anatomy, I found it's really a hard work trying to memorize all stuffs, especially the vascular and nervous systerm, can you give me any suggestinos? Now the exam time is coming, all the contents make me confused very much. Many thanks!
By the way,My major is basic medical science, and I'm also pursuing my doctor dream all the time:)
Hi Khan,
Here are a few ideas:
* Anatomy has a lot of details, but there are higher levels of organization and general concepts, too. Learn those first. For example, before you attempt to learn the action, attachments, and innervation for every muscle in the lower limb, learn the compartments (e.g., medial compartment of the thigh, anterior compartment of the leg). Each compartment has one primary action and is innervated primarily (or exclusively) by one nerve. Once you're familiar with compartments, learn which muscles belong to each one, then learn which ones are the exceptions to the rule. Before you try to memorize specific attachments, learn which joint(s) each muscle crosses. The key is going from general to specific.
* Make reading an active process - diagram, verbalize, make lists of "key words," act out muscle actions, palpate structures, visualize surface anatomy, draw outlines on your own body, quiz yourself, check out what you've read in the atlas or in the cadaver (if available). Take advantage of interactive online resources and do practice questions if they are available. Don't just read words passively!
* Take frequent mini-breaks during periods of intensive studying. If you're really tired, getting a good night of sleep will probably be better for you in the long run than forcing yourself to study when the words have no meaning because your brain is fatigued.
* DON'T PROCRASTINATE.
Hope that helps!
thanks brad:)
I'll try to memorize those things as you've suggested.
Thanks very much and bless myself to get a good score in the exam:)
Interesting post. Perhaps for your next one, you can discuss the distinction between sharp and diffuse abdominal pain, like the pain types you describe in the appendicitis. Heh, I would except I've only had one lecture on it. Keep on posting!
-Avaron
http://scrubnotes.blogspot.com
very interesting blog here
Great post! My wife appreciated the tighty whities:)
Thanks for the detailed explanation. I just recently experienced this for myself.
Having had a colonoscopy done, I awoke from the anaesthetic complaining of left shoulder pain. I was told this was normal. After a few hours the pain would not subside and I was in agony. Of course, they investigated causes such as a perforated bowel, lung embolism and cardiac involvement. Eventually after x-rays and CT scans a torn spleen was diagnosed. That phrenic nerve was quite an interesting experience into learning the secrets of anatomy. I'm still off work (3rd week) recovering from my "day only" procedure.
Keep up the interesting posts. It certainly helped me understand my discomfort.
Oh and by the way, the colonoscopy was all clear. Thankfully.
Hi Brad, I've been very interested in referred pain for a long time. I haven't been able to find any decent references. Any suggestions?
Hi Regan,
Probably the best place to start is a medical anatomy textbook, such as the very readable Gray's Anatomy for Students (by Drake et al.). Neuroscience textbooks (such as chapter 19 in Fundamental Neuroscience for Basic and Clinical Applications by Haines) may also be useful. If you're interested in a particular aspect of referred pain, such as referred muscle pain, you may also want to do a search on PubMed. Hope that helps!
hi brad,
that was really a good post n it gave me a good idea about the weird referred pain...a lot more nerves culprit in all these...ok i will b checkin out this site hope to see more good things ahead...tc
cool blog my friend, im a medical student to, from venezuela, and im in first year right now...
i find really interesting this post...
To Khan W.: I am MS-2 and what helped me not only to memorize but to REMEMBER anatomy (as you always go back to anatomy in your further studies)is to put things into real life scenarios. For example, while learning innervation of the upper arm you might want to right away learn that a fracture of the neck of humerus will damage the axillary n., whereas fracture of the mid-shaft will damage the radial n. There are plenty of good clinically oriented anatomy books. Good luck and don't just memorize, make sense of the information, otherwise you will have to go back later and learn it again.
If only my doctors had known about this before sending me through shoulder surgery, neck surgery, various gastro tests (which came out fine) and a pain clinic.
Finally got to go to Johns Hopkins and they told me what the problem was.
Do you know anything about how to STOP this shoulder pain? JH is telling me I can have the nerve deadend or cut, but I am leery of any more surgery.
I think I'll refer all my former doctors to your page :)
Thank you for writing this. It is EXACTLY what I have (from a fundoplication surgery) and after all these surgeries my doctors thought I was nuts because I was pleading for serious pain pills for the severe pain that would hit me after I ate.
Anonymous, thanks for sharing you story. I'm sorry you had to undergo so many treatments before someone figured out the problem. I'm curious which nerve the surgeons at Johns Hopkins plan to deaden or cut in your case. I'm also curious how you found this web site! Hope things work out for the best.
~Brad
Just a word of thanks from a struggling nursing student who's not only studying for an exam on pain, but really wants to understand and master the subject ...
The appendix referred pain is the same as the reason you have the problem of liver irritation and can give shoulder pain if the midgut did not fully rotate leaving the person with a subhepatic placement of the appendix. This can irritate both the diaphragm and the attending when a patient has appendicitis.
Cheers
a fellow anatomist
enjoy med sch-cool
Thanks for the explanation, fellow anatomist! Anatomical variation strikes again...
Very interesting information. I woke up yesterday with this pain in my shoulder, which I have had in the past intermittently, but usually associated with gas or bloating. Now, I have no other GI symptoms, but I have had this pain non-stop for >24 hours. A trip to the ER yesterday ruled out any cardiac issues, but what the heck is it? I'm also 12 weeks pregnant, so they are reluctant to do further testing. Now I'm worried it could be any horrible number of things.
Thanks for this post. I've known about referred pain for a long time, but rarely read such an easy-to-understand description of it. I have a question about the quality of referred pain. Would you say that the area where the pain is perceived will also be tender to the touch, or is it just that the person thinks that the area would be painful to touch? And would it feel different to local muscle pain in the area?
Hi Ian, My understanding is that referred pain generally feels deep and hard to localize, more like muscle pain than skin pain. Good question for a neurologist or someone who has experienced this kind of pain first-hand. I'll leave another comment if I find something interesting... ~Brad
I have been in excrutiating shoulder pain since mid-September. It started three days before I was hospitalized for a perforated colon due to diverticulitis. Since then I was pain free for only two days -- when I cleansed myself out for a colonoscopy and the day of the procedure. But when I started eating again it came back strong as ever. Because of the perforation, I am having colon resection in two days and am hopeful that the shoulder pain will be gone with the removal of the damaged area. My Dr. thinks it's something else, but my chiro is convinced it is referred pain. I think she may be right. My entire life, whenever I've eaten too much, my right shoulder has hurt. I will keep you posted as to whether it is gone....!
Good luck with the procedure! I hope your chiro is right - certainly sounds like a case of referred pain.
Great article. I have a friend who has pain on the right side of his neck, shoulder and elbow. Sometimes the pain is just in the neck, sometimes just the elbow and sometimes it goes from the neck to the elbow. The strange thing is he has a herniated disc with impingement at C6 on the LEFT side. Doctors say it isn't referred pain. Yet he has no symptoms on the left side. Do you think this is referred pain?
Elizabeth
Interesting case - I'd love to see the images of the herniated disc (e.g., an MRI). Sounds like your friend has a compressed cervical nerve root on the right side, not the left. The pain seems to fit a dermatomal distribution, i.e., a strip of skin innervated by a nerve root at one spinal cord level. Or maybe there's another problem that is unlikely to show up on an imaging study. I doubt it's referred pain but it's hard to say without more information.
Neat blog and very helpful information! We were studying this in vet school too but your page gives a lot of extra, good information, thanks! I'm definately bookmarking his page :)
This happened to me in the days preciding a laprocopic appendicectemy. The doctors couldnt figre out what was wrong with me for 36 hours. It was only when an X-ray was carried out did they realise that there had been a small pocket of carbon dioxide left inside my abdomen. The gas was pushing up against my diaphram causing agony when ever i trie to move eat or breath. I found the whole experience very interesting as i am an occupational therapy student and have been studying anatomy. great blog by the way
I've had the shoulder/scapula pain thing on and off for years and self-diagnosed it as gastrointestinal since a burp or passing of gas always relieved discomfort. Same thing for my own and family members' experience of other miscellaneous, occasional not-otherwise-explained aches and pains in joints. Finally, an MD confirmed I wasn't nuts. Sometimes heating pad to the belly area helped. For the past two weeks I've been having somewhat diffuse lower back ache and suspect it's the same cause, but getting worried it might be symptomatic of more serious trouble. Thanks for article and any insights.
Brads- great blog really helpfull. Im just starting a medical field and currently taking APII. We were discussing referred pain and I was amazed that neck pain could be a referred pain for liver or gallbladder problems. I've had neck pain for six months. I've also had a pain in my URQ and can palpate that area to create it. Though Ive had CT Scans, Hyda-scans, X-rays, MRIs on the head and neck(c1-c3)-All results were normal. Neurologist diagnosed severe muscle tension, so Im currently doing a series of BOTOX injections. Should I mention this referred pain suspision to my Nuero? Thanks for you help
Hi Dawn,
If you can actually create pain in your neck by palpating your right upper quadrant, that certainly sounds like a case of referred pain, and yes, I'd bring it up with the neurologist. I'm guessing that a lot of potential problems have already been ruled out by the imaging studies, but who knows, your doc may want to take another look...
Brad
I have 2 questions at the end. But, I thought I'd contribute some additional examples of referred pain...an older family member was seeking treatment for severe hip pain for a while before learning that it was referred pain as a result of prostrate cancer. My mother had shoulder pain for a while - her GP diagnosed an encapsulated shoulder and sent her for physical therapy. It turned out she had lung cancer. I've had referred pain in my right upper back from right upper abdominal pain (which only recurs if I've eaten too many cashews or have Starbucks a couple of days in a row). I also have a pain in my left shoulder that I assume is from a couple of herniated discs I have between C5,C6,C7. When this flares up, I also have the numbness and tingling in 2 of my left fingers. They call this radiculopathy - but, is this different from referred pain? And, my last comment/question is regarding what I was searching for when I ran across this site - I've been having middle abdominal discomfort and tenderness and I also have a large left ovarian cyst (endometrioma) that I'm supposed to be scheduling surgery for. I've been having more frequent pelvic pains and thought if the abdominal pain is related that I might should get my dr to hurry along with scheduling the surgery since there is a concern the cyst could lead to ovarian torsion or rupture. Thanks,
Hi Tanya,
Interesting examples of referred pain, especially the upper back pain from eating cashews! I'm not totally convinced that all of the cases you mention are referred pain. For example, the severe hip pain could be due to prostate cancer that metastasized to a hip bone (sacrum, pelvic bone, etc.).
Radiculopathy isn't considered referred pain, because the direct injury of nerve roots that carry sensation from the affected body parts (in your case, the upper limb) can explain the pain (and numbness and tingling).
Regarding your last question, unfortunately I'm not qualified to give medical advice, but I can say that when pain increases in frequency or intensity, it's reasonable to be concerned and express those concerns to your doctor.
Brad
Talking about referred pain,for the last 4 days I could not sleep at all because of a back pain that would extend all the way to my testicules, could not sit or lay down on my back even in the ER.
Turns out to be peptic ulcer.
By the way ,great deal of relief - a hot shower every 1/2 hour
I am so impressed by your responses to such various posts.
I found this by searching google for referred shoulder pain, based on my own intense shoulder pain that is unexplained by bursitis or anything else logical. I am 28 years old and i am otherwise healthy, but at this point i am out of my mind, i would take anything to make it stop. This morning upon being woke up by the pain (it gets worse when i sleep, no matter how or where i sleep) my right side became so painfull, it reminded me of when i was in labor for 13 hours. I couldn't breathe. I finnaly drug myself out of bed and went running for the bathroom.
I think i may have gallbladder issues, and your blog was very helpful and even a little reassuring, if nothing else, that i am not crazy. This shoulder (right side) hurts in such a deep unexplainable way. I have taken alieve & tylenol at my doctors advice to reduce inflammation, and i have tryed creams. Hot showers seem to help, but not much. It is just so deep. My husband offered to rub my shoulder but i refused fearing any touch, but it turns out, it doesn't cause more pain to touch it. I can't tell you how deep this pain is, it's all i can think about. I feel like a crazy person.
I don't use any medications, and i try to live healthfully, yet i could crawl into the ER right now and beg for drugs. I feel like they would laugh at me. I am desperate, and was going to go to a chiro, except i don't want my neck manipulated, too much risk there.
Anyway, sorry for the long post, just wanted to say thank you for shedding light on this for me.
To the poster above, typically referred right shoulder pain from the abdomen is caused by irration of the diaphragm by the gall-bladder, liver, or duodenum (first part of the small intestine), although anything that lies in the right side of the abdomen can cause it.
I would ask your doctor about referred pain, and about what tests might be applicable. The sooner you get to the bottom of it, the better.
Thanks for the article Brad; it was very helpful in clarifying some things. I came across it when trying to find out why referred pain from the diaphragm is always shown over the right shoulder in the textbooks and never the left.
Cheers,
Tim
First year med.
Great website. I have been dealing with a pain in my upper left shoulder blade area which began almost one month ago. The pain has now traveled to my left side neck, right side shoulder and right forearm +elbow. Both hips at the joints have now began to experience pain with the right side being more significant. Feels muscle related. I've been to two GP's a Chiropractor and PT. Any advice would be so appreciated.
Deb, I'd recommend seeing a neurologist, ideally one that specializes in pain management. He/she will ask you a lot of questions and probably order various lab tests and imaging studies in order to figure out the problem(s) and hopefully make it better....
Very interesting, very useful -- thank you!
You might be interested to note that referred shoulder pain often afflicts women with OHSS, Ovarian Hyperstimulation Syndrome, a common (but often unrecognized) complication of fertility treatments. Fluids build up in the abdomen and I guess must irritate the diaphragm/splenic never. Hurts like the dickens.
Best wishes with your med school career!
Found your site on a google search for phrenic nerve referred pain. I had this happen this weekend, so bad I thought I had a pinched nerve and called my doc who sent me to the ER. Turned out I had pneumonia which quickly turned into a pleural effusion. Several days in the hospital, I am back home and still very ill and the pain is horrendous. Today it moved to my fingers as well and was just trying to find out if that is typical, its the top of my hand and my fingers that are tingly and painful. Docs keeping a close eye on me, just hate to be a constant complainer if its just part of the whole thing! Great site, thanks for the info.
this is excellent info thanks for your site, Brad. Would like to know if you have come across gouty like R. big toe/ ball of the foot pain (stabbing-like) referred from LLQ from symptomaticDiverticulosis or Mild Divertic.-itis? L.Toe/ball of foot pain not as remarkable as the Rt. i am not diabetic. thanks
Thank you for the illustration. I have a book that my school gave me to learn about "red flags", but it didn't give a good description of the referred pain patterns.
The illustration you posted is incredibly helpful and I will use it throughout my career in physical therapy.
If only my doctors or I had read this three years and several thousands of dollars later. I had a right rotator cuff injury. Extreme pain has dogged me ever since. I never put it together with eating. Just yesterday I had my stone filled gall bladder removed. The doctor was amazed that I was not feeling the pain in my gall bladder area. Sorry your knowledge came late for me.
sweet... thanks for the help !! lots of good information!
Brad, I was diagnosed with Chronic Myofascial Pain 8 years ago. I see an amazing physiatrist for pain management and have read as much as I could over the years. It is always stated, in anything I have read, that the pain I have is referred pain, but it is never fully explained. I understand what referred pain means, in a general sort of way, but I am curious as to the how and why. Could you explain further please?
Interesting stuff.. when I need to burp I often get pains in my left upper arm or even my hands!
I am a 24 yr old female. I have an increased body temperature, normal HR/BP, gas and abdominal distention WITHOUT pain. My pulse is strong and can be felt in my abdomen. Sometimes I have constipation or diarrhea and severe lower back pain (worst when I try to sit up from lying postion - get about 45 degrees before collapsing). Rarely I have sharp (not crushing) chest pain. These symptoms do not occur in conjuction with or without food intake. Any guesses?
Hmm, this isn't a lot to go on, especially for someone with very limited clinical experience (like me), but I wonder about an inflammatory bowel disease like Crohn's disease or maybe ulcerative colitis. Other possibilities are irritable bowel syndrome, celiac disease, infection...and I'm sure there are many others, since abdominal problems can be notoriously hard to diagnose. Probably your best bet is a visit to a doctor. Good luck!
Hi Brad, I just had my gallbladder removed 3 weeks ago. My gallbladder was very inflammed and I also had a stone. A few days ago my old original pain came back. The pain is just below my rib on my right side and extends into my right side and back area. My doctor ordered another URQ ultrasound and also a hepatic screening. Got the results today and everything is normal. Doctor says that my pain cannot still be from my gallbladder or from my common bile duct as the ultrasound showed nothing there. To say the least, I'm very frustrated and concerned. I was told that the pain i was having was because I needed to have my gallbladder removed, and now I have the same pain back! Any words of wisdom or advice? Thanks so much Brad!
Hi. I posted earlier about shoulder pain etc. Yesterday I awoke with weird pain laterally under bottom right rib. I massaged area to ease pain and, once again, it triggered burping and some relief. Sometimes pain tends to stick around for a few days even after what I believe is entrapped gas has been eliminated. Still achy today, but less.
Hi Brad: Great article....I've experienced intermittent pain (and it is excruciating) since I was about 15 years old (20 years now). It lasts for anywhere between 15 and 45 minutes and completely incapacitates me. The pain usually starts in the jaw and quickly moves to my chest to where it feels like someone is pushing knives into my chest and back....sounds like fun doesn't it?
I can sometimes predict the pain based on my posture. It always occurs after I've been slouching in my seat or on the couch. Since its only monthly I've largely just ignored it. Frequency has not increased over this time period.
Any thoughts?
Wow, I would take that pain very seriously, especially since it incapacitates you and it apparently mimics the pain of a heart attack and/or aortic dissection (neither of which is likely in someone your age, but still possible). See a doc.
Hey Brad,
I posted on 6/26. I'm the one who had my gallbladder removed and am still experiencing pain in my RUQ under my rib cage and into my side and back. Do you have any thoughts or comments? Thanks!
I had a bower resection 5 wks ago and for the past 10 days have experienced referred pain in the shoulder. I can find lots of info on what causes this but almost nothing on what to do about it. Tylenol doesn't touch it, nor does ibuprofen, and I'm going nuts! It's keeping me awake which can't be good for healing. Any sugestions?
Anonymous on 7/11:
If I were talking to you in a clinic, I'd want to know more about the history and nature of your pain, both before and after the cholecystectomy - you know, when did it start, quality and severity, is it associated with any activities, what makes it feel better or worse, continuous or intermittent, etc. Although it seems unlikely in your case, it's possible that the RUQ pain is unrelated to your gall bladder or liver. For example, I'd wonder about a kidney stone, or maybe retrocecal appendicitis. Depending on what you told me about your history, I'd consider more imaging studies and labs. As always, the best advice I can give is talk to your doctor, and get a second opinion if you're not satisfied.
Anonymous on 7/12:
You should definitely talk to the doctor who performed your procedure. If ibuprofen and Tylenol aren't working, he/she might write a prescription for a combined opioid/acetaminophen analgesic like Percocet or Lortab. Other options such as certain antidepressants and anticonvulsants are available for chronic pain, but hopefully your pain won't hang around that long. If you're not satisfied with your current doctor, you might consider getting a referral to a pain specialist.
Of all the hits for referred pain, yours is definitely the best site. I've been curious about whether severe pain in my left teres muscles might have been referred pain from a stromal tumor in my small intestine. Especially on long drives, the shoulder pain was unrelenting and, even tho it didn't help, I took lots of ibuprophen - enough to make the tumor hemorrhage (and be found, fortunately). After surgery to remove the tumor, it took more intervention to stop the shoulder pain, but I thought it could be a reflex pain arc, like in reflex sympathetic dystrophy. Do you think there might be a connection?
p.s. love your booklist. Vermont's loss is Utah's gain. Best wishes with school, and then please return to VT. :)
Hi Blue429, I'm glad you've enjoyed the site! Upper back pain from a GIST (gastrointestinal stromal tumor) in the small intestine seems unlikely - abdominal pain is a more typical presentation. However, GISTs are most common in the stomach, which could definitely lead to referred pain in the upper back (perceived, perhaps, as teres major pain). I'm curious about the precise location of your GIST, and whether an additional site in the stomach was definitely ruled out....
The tumor was defintely in my small intestine. Initial dx was bleeding ulcer, but my stomach was quite healthy. I had a few months of vague symptoms (fatigue, diarrhea) but I don't remember any abdominal pain. The outer border of my scapula was tender to touch so maybe it really was a coincidental muscle strain.
Great info, many thanks, I have just had my right ovary removed due to a fist sized dermoid cyst, I have had severe but interrmitant right shoulder pain since. The nurses and docs who treated me all advised in various vague ways that it was referred pain due to either irritation of the diaphragm or due to the gas used - they had tried to remove the cyst by keyhole surgery initially and the gas can sometimes take days to work its way out. What do you think? It has felt almost like a trapped nerve as at times my whole arm and fingers have tingled with the pain.
They have siad it should just last a few days and that walkign around sometimes helps.
Gr8t Brad!!! I was also trying to figure out why the periumbilical pain in appendicitis occurs there anly and not along its roots! After reading ur blog it made sense that somethings cannot be explained why as to that particular site only and not the whole course of the nerve!! Thanx
Ok, I am so glad that you wrote about referred pain because I learned that in school. I have an issue where I have a bad headach accompied by gas. I always thought that maybe I was having a migraine.
Everytimne I would touch a certain part of my head where the pain was, I would burp. It is very annoyiny and I worry all the time about the food that I eat. Thanks again for the info
I think your blog is great, and I would like to feature you on the new
Wellsphere. We feature only the best health bloggers on our WellPages,
which are special pages that our Health Knowledge Engine crafts to give
our users answers to their health questions. We would feature you on all
the pages on topics that our knowledge engine finds are related to your
blog postings. Because we have over 2 million visitors each month (and we
are growing rapidly), you would benefit from an expanded audience for
your writings. If you would like us to feature you, send me an email to
Dr.Rutledge@wellsphere.com
Cheers, Geoff
I have been experiencing shoulder pain for about a month. In the past month I have tried all kinds of pain relief. Last night, I experienced an evening of loose bowels and today my shoulder pain is gone. I thought that was really curious until I remembered that my friend had a spleen injury that was diagnosed by shoulder pain. I am assuming that whatever was making me have the loose bowels had been building up and now that it has passed, that relieved the pressure on my spleen. Thanks for the blog, I am going to monitor life and if my shoulder flares up again, it is off to the doctor.
great illustration for a normal person (not Doctor) to understand. I have had a terrible persistant pain in my right shoulder and neck.. Finally I've been diagnosed with celiac and my gallbladder is going to be taken out next week. I hope it goes away. Do you have any suggestions for referred pain from surgery I've had in the past? I had my head cut and my face peeled back to remove a bone growth from the oribt of my left eye. My scalp and forhead have never been the same. It has been about 7 years. Headaches and nerve pain bounce all over my head. thanx for such a cool website
Thank you for this very interesting website. I have had shoulder pain for a few months now and mentioned it to my gyn. He ordered a catscan and found a mass in the upper right quadrant of my abdomen. I underwent a second CT yesterday and now will wait for further results. Interestly enough, I mentioned the shoulder pain to the surgeon and he said there was no association; The gyn disagreed and I agree with the gyn as I have had no pain the abdomen thus far and was shocked to find the problem in the abdomen. Keep up the good work. AHB
Hi Brad,
Useful article. Just two questions, what nerve causes referred pain to jaw in myocardial infarction? And why does pain from angina and MI not manifest in the right side of the body as well as the left?
Cheers
Vin
Vin,
1. The mechanism of referred pain to the jaw in MI is still unclear, but recent evidence points to involvement of the vagus nerve (http://www.nature.com/bdj/journal/v204/n4/abs/bdj.2008.101.html).
2. Actually MI pain *can* radiate down the right arm, but that's much less common than the left. I'm not sure if the heart is more heavily innervated by left-sided pain fibers, or if the left side of the heart is more likely to be affected in a heart attack. Or maybe there's some other explanation.
Another interesting point is that, for reasons unknown, women are less likely than men to report chest pain in an MI (http://archinte.ama-assn.org/cgi/content/abstract/167/22/2405).
Thanks for this wonderful website. By the way, could you please tell me why visceral pain in the spleen is referred to the hypochondriac region as supposed to the epigastric region? Thanks again.
Thanks for this wonderful useful article. My mother was complaining of Right Illiac Fossa heaviness. All relevant Investigations were negative. Finally diagnosed as referred pain of Sciatica!
Now under treatment for Sciatica. Hope this information is also useful.
Hello. Back in 1999, I had a fundoplication for gerds, which worked well. In the last year, I have started to suffer from severe back neck pain,esophageal pain, and pain from below the tip of my sternum to mid sternum. I was checked out for gallstones, and liver issues but nothing. A barium swallow was performed, but no incidence of swallowing problems such as reflux were found. Endoscopy was performed and my fundoplication was found to be loose, and I have a 4 cm hiatal hernia. Could this be putting presure on my phrenic nerve, causing me massive headaches,esophageal pain, and swallowing pain. Oh yes, one more thing, heart disease was also ruled out. I am just about at the point where I want to call in Doctor Kavorkian. If you have any suggestions please email me at lily_darcey@yahoo.com
Hi Lily, it sounds like the most likely source of your pain is the new hiatal hernia. Anatomically, the vagus nerve is more likely to be involved than the phrenic nerve, but either way, I'd recommend talking to a surgeon ASAP about the possibility of repairing your fundoplication. Also, if your pain gets a lot worse and you start feeling really sick, you may have a strangulated hernia, which is a surgical emergency. See http://www.emedicinehealth.com/hiatal_hernia/page3_em.htm for more information.
Don't underestimated shoulder pain if im not mistaken..
Great post Brad! I was "pimped" by an attending on how many causes of right shoulder pain I could think of and basically mumbled my way through a random sampling of things you've included in this post. And I'm just a 2nd year med student, so you can imagine how intimidating that was. It's one of the experiences I'll definitely be adding to a blog I've decided to start up at http://themedstudentexperience.blogspot.com. I plan on looking back at my first two years as a med student. Any advice on year 3 clinicals? Thanks, man!
Brad, this is a great blog. I had a routine colonoscopy 2 weeks ago. Day after the procedure I had incredible left shoulder pain. In the last 2 weeks I have probably had only 2 nights of full rest. The pain makes me get up. Called doctor to let him know of my pain 5 days after the procedure. They basically blew me off. I called again 3 days later. In the meantime, I was experiencing numbness down my left arm and in my outside two fingers. I can't tell you anymore if the pain is linked to the original pain I was experiencing or if it is now something else which causes the numbing. Tomorrow I will see a nuerologist (previous appt. for monthly headaches)and my internal med doctor who "talked" me into the colonscopy. I will be asking if air was injected in the bowel during the procedure (which may have caused the original pain) but then the numbness has me stumped. Any suggestions? Thank you very much.
Med Student Experience, probably the best advice you can get is from 3rd and 4th year students at your school. In general, my MO is to show up, have a positive attitude, learn as much as I can, and treat everyone with respect (especially the patients). I'm also completely up-front about my career goals, e.g., I don't pretend that I'm considering psychiatry just because I'm doing the psychiatry rotation. Clinical evaluations are so subjective that I've stopped worrying about them.
CJ, I think you're doing the right thing (talking to your doctors). I'm not sure what to make of the numbness in your case - it doesn't fit the classic picture of shoulder pain that you might expect after an abdominal procedure...
Brad, just a followup to my post on 1/18 and your reply on 1/19. I went to a nuerologist and internal med doctor. The nuerologist brought up the referred pain, which I was glad to see. He put me through some stretches, etc. and he could locate the approx. source area of my pain in the left lower shoulder area. So he ruled out referred pain. I have been on steriods this week (pills only) and I still have some pain (not piercing as before) in the back and numbness down the arm and fingers. Sleeping is difficult but better. I will call on Monday to let them know how the steriods are/aren't doing. Perhaps I will have to live with this...I hope not...but I can still function, at least. This followup is to help anyone with a similar situation and what was prescibed for me. Your comments, Brad, are appreciated as to if I need to ask a specific question of the doctors.
Great article. Was searching for referred pain b/c my lower jaw is hurting very badly and, although I have teeth problems too, I realized it is hurting b/c I have yet another ear infection. I'm 28, have a tube in my right ear and it still gets infected quite often.
In another example of referred pain, at the very end of my pregnancy (on my due date!)I began having incredible pain deep in my chest, abdomen, up to my neck, shoulders, down my arms and into my hands. Was initially diagnosed with "gas" as I was not currently in labor. Five days later, after giving birth, the same horrible pain persisted. Two days later, after ruling out gallstones, I was finally diagnosed with HELLP Syndrome. The extreme pain I was feeling was my liver...
this note is very interesting. i have unbearable sharp periumbilical pains that come and go every 6 months or so but ive never been able to figure out why, yet ive had a constant right shoulder pain for 7 years without explanation.
yeah thats fine, but they say the pain in my neck ( I have bulging disc and lump in neck ( is referred pain....from where...my neck??? hello....it catches when i turn my head.. I hardly think this is referred pain from anywhere else....??/lol
oh doctor that's was extremely helpful..
thank you =D.
hye Dr, im diagnostic imaging student from Malaysia, your article seem interesting to me. could you post a note regarding right iliac fossa pain, maybe i will get some idea to choose best modalities for different diagnosis at this area.
Hi Ro, I'm not sure what you mean by pain in the right iliac fossa - is the patient experiencing pain in the right lower quadrant of the abdomen, or right flank pain, or deep pain that seems to be centered on the iliac fossa, or something else? My first thought is musculoskeletal pain, since as you know the iliac fossa is filled with the iliacus and psoas major muscles, but there are many other possibilities, including appendicitis, kidney stones, IBS, IBD, herniated disk, abscess, etc....
Great post. I have suffered from referred pain for over 20 years. I have had every type of test done, and all results were negative. As my doctor once said, "the good news is that we didn't find anything, and the bad news is that we didn't find anything". I have consciously decided that my pain is like a confusing "traffic jam" of brain signals, that I cannot seem to turn off. I know that some day there will be a simple "reset" button for the nervous system. Until then, thank you for trying to explain the unexplainable. S
HI
I HAVE A TEAR IN MY ROTATOR CUFF..STARTED PI, BUT NOW HAVE A INFLAMED BICEP....BESIDES THE PAIN IN THE SHOULDER AND BICEP, I HAVE PAIN FROM MY THUMB TO MY ELBOW...COULD THAT BE REFERRED PAIN OR ANY INDICATION OF SOMETHING ELSE. THE PT SAYS MAYBE.
Hi Anonymous, my best guess is that something (perhaps related to the inflammation of your biceps) is irritating or compressing your musculocutaneous nerve. As its name implies, the musculocutaneous nerve innervates both muscle and skin. The muscles controlled by the musculocutaneous nerve include two major muscles that bend the elbow: brachialis and biceps brachii. The skin innervated by the musculocutaneous nerve is a patch on the lateral forearm (from the base of the thumb to the elbow, as you described). If I were examining you, I'd want to figure out what's bugging your biceps and, perhaps, your musculocutaneous nerve...
THANKS BRAD....NOT TO BOTHER YOU AGAIN, BUT WHAT CAN I TELL MY ORTHOPEDIST THAT WILL MAKE HIM UNDERSTAND ITS NOT REFERRED PAIN FROM THE ROTATOR CUFF?
THANKS AGAIN FOR ALL YOUR HELP
I should clarify that I don't know whether it's referred pain or not. To figure that out, your orthopedist needs to get a detailed history and perform a careful physical exam. You could ask him/her about the possible involvement of the musculocutaneous nerve. An EMG might help.
THANKS....IM SEEING HIM N/W...IM SO GLAD I FOUND YOUR BLOG.
THANKS AGAIN
Brad,
What a brilliant article. Referred pain is such a hard concept to grasp and diagnose. I have had left shoulder pain for a year. After clearing my heart(angio), neck(mri) and shoulder(injections, xrays); I am sure it is referred pain. I also have a lap band with a hiatal hernia on top of the band. I have terrible L shoulder pain and my surgeon who did the lapband refuses to attribute this to referred pain from the phrenic nerve (from lapband and hiatal hernia). I am trying to convince him that maybe the band is misplaced. Good Luck finishing up Med School!!! As a nurse we need more good Docs. Have you chosen a specialty?
Erica
It is really great to know things. Even better when shred with others. Thanks for sharing.
hi there...
i always had a feeling of pain that i could not describe just below my umbilicus since last year...i also feel pain in my left lower quadrant of my abdomen whenever i defecate...so i went to a hospital here in our place for a check up and i was diagnosed through ultrasound...but my ultrasound has shown normal internal organs except for a small ovarian cyst...does the pain that i feel just below my umbilicus suggests an ovarian cyst or could it be something more?....
Erica829, thanks for your comments. I'm most likely heading into radiology.
Anonymous on 4/28, sorry for the delayed response - things have been busy in the ICU. Pain just below the umbilicus is certainly consistent with an ovarian cyst - in fact, that would be a nice example of referred pain - but cysts aren't always painful and something else more serious could be the source of pain. I'd go see a primary care doc if it's not improving or you develop new symptoms, such as blood in your stool or fever/chills...
I wrote you back in November of 2008. Since the second catscan, I had a huge mesenteric cyst removed and my referred pain has gone away. The Florida Hospital South surgeo was familiar with referred pain. Thanks for your blog.......I am now in good health.
I have abdominal pain, swelling, and burping which can be triggered by my physical therapist working on the lower left quadrant of my back. I am assuming from your diagram that I need to see a Dr. to have my kidneys checked. Am I right? Any other ideas? By the way, abdominal CAT scans, xrays, and stomach emptying tests have shown nothing. This is why I am trying to follow the referred pain to find the answer.
Hi anonymous, I haven't heard of abdominal symptoms being triggered by physical therapy. Have you experienced other symptoms that suggest kidney problems, like blood in the urine? Any fever or other symptoms suggesting an infection? The absence of findings on abdominal CT is reassuring, but it's still a good idea to see your doctor if you're concerned.
I was very interested to read this blog post. For months Ive been suffering with pain in my right shoulder area, and lower right back area (exactly where you diagram shows the livers referred pain to be). I paid a fortune to see an osteopath thinking it was back trouble. But eventually I got so ill that I went to hospital and tested positive for hepatitis in my liver. So the referred pain was exactly spot on for your diagram. Although by the time I got to the hospital stage I was also experiencing a lot of chest pain too.
Hi,
Can you help with an explaination for this type of refered pain...
Pressure is applied to the region of the peroneous longus and brevis, resulting in localised pain (obviously) and an "itchy, prickly" type pain in the lateral chest wall in the rough vacinity of the 12 rib, to the lasing extent tat it needs to be scratched by the subject.
Would be evry inteersted in some theries and if possible, some follow up articles.
Does it have something to do with embyonic developmnet of the feotus inutero? Just grasping at straws!
Thanks
Alex
Hi Alex, interesting observations that I haven't heard before, and I don't have a good explanation for them. Probably related in some way to embryological development, but I could only speculate. Have you seen this finding in more than one subject?
Hi Brad,
The subject is me in this case, but I have seen this in other subjects also.
Still baffled by this. Asked my A&P lecturer and he says he is unsure of the cause. We discuss dermatomes but agree we may be close, but no prize yet.
The only thing I can find courtesy of Google is on a website discussing "Axon Reflex"... http://medical-dictionary.thefreedictionary.com/axon+reflex.
What is you thought on this though process. It states...
"axon reflex -
a neuron reflex in which an afferent impulse travels along a nerve fiber away from the cell body until it reaches a branching, where it is diverted to an end organ without entering the cell body. It does not involve a complete reflex arc, and therefore it is not a true reflex."
So, maybe some sort of reflex arc just a little wayward. Perhaps a crossed neuron or synapse.
Maybe, consider something a little more off base like a reflexology type response.
What do you think?
Alex
Very interesting and helpful. I had cancer, surgery followed by radiation through the intestines and ended up with celiac disease that was undiagnosed for a long, weak, declining, scary year. Three years later, energy continues to return, although slowly. If I get tired or eat something that has been gluten contaminated, it's between the shoulder blades that I'll feel it first, and then in the ball or big toe joints of my feet. Weird, but true. Three to five days later, things will have settled down, but the last thing to go will be the dull, throbbing pain in my feet and between those shoulder blades. So glad I'm not crazy, and that it's all likely related to the same original difficulties. Weird, but reassuring.
how about pain in the inner part of both thighs?
Groin pain can actually indicate a problem with the hip: http://orthopedics.about.com/od/hipknee/g/groinpain.htm
Any unusual physical activity recently?
Brad,
I have a question for you like everyone else. I am having deep pain on my left side (more towards the front than back) just below my rib cage for 3 days. I hurts when I breathe. Any suggestions?
Hard to say without a little more information (and probably a physical exam, too). Medical students are taught to characterize any complaint of pain in great detail, for example using the mnemonic PQRST AAA:
* Position: Where is the pain?
* Quality: How would you describe the pain?
* Radiation: Does the pain radiate to other parts of the body?
* Severity: How bad is the pain on a scale of 1-10?
* Timing: When did the pain start? Was the onset sudden or gradual? Does it come and go? Is it getting worse or better?
* Alleviating symptoms: Anything make it better?
* Aggravating symptoms: Anything make it worse?
* Associated symptoms: Anything else related to the pain?
The answers to all these question can narrow down the possibilities substantially, but a definitive diagnosis may be elusive without an exam and possibly lab tests and/or imaging.
For now I'll say that left upper quadrant pain (i.e., the location you're describing) can be caused by many conditions, including gastritis, gastroenteritis, pancreatitis, peptic ulcer disease, splenomegaly (big spleen, e.g. in leukemia or lymphoma), ruptured spleen (e.g., in trauma or mono), left lower lobe pneumonia, various kidney problems, etc. If you're young and basically healthy, it could just be a simple musculoskeletal problem (e.g., a "growing pain") that will go away on its own. As always, if you're concerned, I'd go see a doctor.
Thank you for the blog. I had a lap nissen fundoplication almost 7 weeks ago. I had the usual general shoulder pain for a few days from the gas used in inflating the abdomen. That dissipated, but I continue to have pain in my left shoulder (actually my upper trapezius) in an area that is about the size of of silver dollar. On palpation, the area feels like a muscle spasm in that it is a painful lump. But I have never heard of a muscle spasm that lasted 24/7 for 7 weeks. The surgeon that did the fundoplication doesn't have any kind of answer. Its sort of a "in some people the pain lasts longer" answer, with more pain meds. It has gotten worse over the last 2 weeks, and is affecting my shoulder joint; I had a shot for AC joint bursitis last week. The orthopedist who did that has referred me to a chiropractor to see if he can figure it out, as well as to PT. I'm not sure why it is my left shoulder, since your illustration said it was the right. All three doctors (my GP, too) don't seem to register a problem when I say it's my left shoulder. I'm now on pain meds, valium, and I have to use a TENS unit as well, and with all that, I get only partial relief. Does all this just sound like referred pain from the diaphragm?
Gretchen, what you're describing doesn't sound like a typical case of referred pain, but I can't rule it out. Certainly the timing and location of the pain make me suspect the pain is related somehow to the Nissen. You might talk to one of your doctors about getting a CT or MRI of the surgical site (and maybe the shoulder too) to make sure they aren't missing something.
well this is frightening.
for the professor who died of cancer, does routine blood screening help you determine whether a patient has _any_ kind of cancer? or are there cancers that won't show up that way at all?
Hello, and thanks for the information. I have had pain in my left shoulder for well over a year. It comes and goes and nothing I do makes it feel better or worse. I have tried to find some kind of pattern or cause and nothing that I can find makes it start or stop. I went to multiple doctors and got an MRI of my shoulder, and multiple x-rays and there is nothing structurally wrong with my shoulder except some extra mobility or looseness in the joint. I also tried physical therapy which didn't have any effect on the pain. When the pain hits its peak, it sometimes make my vision go out of focus. It feels like the pain is coming more often, and staying longer, and getting worse, I feel like I am going to lose my mind!! The pain definitely gets to a 10 often, and I have tried heat, ice, icy hot type items, advil, tylenol, and nothing helps. What should I do next? Any help would be great!
Thanks,
Gina
Scout: Unfortunately there is currently no safe, inexpensive, effective way to screen for all cancers. Screening is only recommended in certain age brackets for a few relatively common, treatable cancers (e.g., colonoscopy, mammography).
Anonymous 8/20: Your pain has several concerning features, including its intensity, resistance to conservative treatment, localization to one region, and trajectory (getting worse). Given the lack of findings on shoulder imaging, I would definitely think about referred pain from another site like the base of the left lung or the left upper quadrant of the abdomen. Have you discussed this possibility with any of your doctors?
Brad, this is to follow up on my note of 8/15. It appears that my shoulder pain is only indirectly because of the fundoplication surgery. It seems I have had a trigger point in that shoulder for years (and yes, I have had some muscle spasms there before, but never this bad.) I think that the post surgical shoulder pain activated the trigger point in a way that it has never been before. It has basically been in non-stop contraction for 2 months. Understandably, this very painful condition has affected my shoulder joint as well. I am finally getting some relief with acupuncture, but I am holding out the possibility of a trigger point injection if I can't get total relief through more conservative means. Thanks for your input. All input helps when you are trying to solve a puzzle.
Dude, rock on. Thanks.
For the last 3 months I had pain between my shoulder blades now my whole back hurts from my neck to my hips my doctor has sent me physical therapy but no help at all. Any ideas what this could be? Also my sciatica is getting worse.
Hard to say without knowing more about your history. One condition that comes to mind is polymyalgia rheumatica...
Hi Brad, first year medical student here (UMDNJ). Found your site when doing a quick refresher on referred pain for an MI (#1 site that came up on bing search). Your post was very helpful, thanks. Also, from what I have read, angina pectoris doesn't seem to produce referred pain like an infarction. Is this simply because the pain is less severe? Is it because angina pectoris results from lactic acic buildup whereas an infarction is from tissue death? Do they both result from lactic acid buildup?
Interesting question about the pathophysiology of angina pectoris vs. the pain of myocardial infarction. I'm not sure if anyone really knows the answer: "The exact mechanism by which ischemia produces discomfort is unclear but may involve nerve stimulation by hypoxic metabolites." (http://www.merck.com/mmpe/sec07/ch073/ch073b.html)
I was reading an article online about brain disease. I don't understand the cause of the spinocerebellar degeneration disease. If the cerebellum is slowly decaying, how does that directly correspond to comas?
I'm currently considering to enter med school. Do you think this software would be helpful?
http://www.squidoo.com/easyhumananatomy
Anatomy is not that much tough as if it looks when you happen to be got taught by very experienced doctor Dr SHM Abdi, who also taught in Africa, India (KGMC, AMU, ERA) watch his video lectures at http://wacky5.com/video-lectures-of-anatomy-by-dr-shm-abdi-at-eras-medical.html
To follow up on my note on 9/10. I am a 56 year old male and for the last 3 months I had pain between my shoulder blades now my whole back hurts from my neck to my hips my doctor has sent me physical therapy but no help at all. My doctor also sent me to a Hematologist at a cancer center and they found nothing out of the ordinary on my blood work. I have also had a CT Scan of my brain and it was normal. And I have also had nuclear heart stress test while walking on a treadmill and was normal. They have taken x-rays of my back and found arthritis in the upper and lower parts of my back. Also I am seeing a kidney doctor at this time. I have seen a chiropractor after a few x-rays he adjusted me and I have had some relief from my back pain and have helped my sciatica a little. I have smoked off and on for 30 years. I may cough maybe once or twice a day or on a bad day 3 or 4 times a day. Some times I might cough a little green stuff up but it’s very little. So could COPD be the cause of my back pain or maybe something worse.
To the man with pain between your shoulder blades. The vagus nerve, connects from the stomach to the spine. I had an ulcer hurt in that place, referred pain, no doctor could find out what was wrong and two months later the ulcer perforated, Causing peritonitis. Ask for an indoscopy to find out if you have an ulcer. I had to have explorotory surgery.
Many thanks - this is highly readable! From a second-year med student in the UK
HI BRAD-I HAVE A SHARP PAIN UNDER RIGHT SHOULDER IN THE BACK AND IT FLARES UP DURING NIGHT TIME AND AT THE SAME MOMENT I GET STOMACHE PAINS AND FEELING SICK AND GETTING SICK IT LASTS AROUND 3 HOURS,THE PAIN ALSO GOES FROM RIGHT SHOULDER IN THE BACK TO NECK AND SHOULDERS WHICH IS A BURNING FEELING AND WEAKNESS.can you help cheers
Anonymous, do you ever experience that pain after a meal? Your description is consistent with a bad case of gastroesophageal reflux disease (GERD). However, it could be something else - I'd strongly recommend seeing your doctor.
hi i really found this blog useful, however i would like to ask you how one can distinguish between somatic and visceral pain.
thanks for your help!! :)
In general, somatic pain is sharp or burning and easy to localize. Visceral pain is more dull, diffuse, and harder to localize. However, these are just general patterns; there may be exceptions. Also, other types of pain like neuropathic pain may not fit neatly into either category...
I am a PT who specializes in treating pelvic pain/dysfunction. Post-hysterectomy suprapubic area pain that is episodic in nature. Spreads across entire lower abdominal area, at the worst 9-10/10. Described as "deep", "dull". Normal bowel function, urinary frequency that has improved to WNL's with diaphramatic breathing/relaxation training. Gets worse with stress. Negative for connective tissue dysfunction, myofascial tender/trigger points pelvic floor muscles/oburator internus both internally/externally. Hip active/passive ROM WNL;s. Pretty bad MRI for lumbar/lower thoracic disc involvement but no central stenosis. What are your thoughts? Referral from lower thoracic segments? - something I have rarely seen if at all. Post surgical scarring/adhesions? Pt. has had some abdominal MFTRP that we are treating.
As far as I know, deep dull lower abdominal pain after a hysterectomy is most consistent with surgical injury of pelvic tissues including visceral nerve fibers, and perhaps, as you suggest, post-surgical scarring. I doubt the degenerative disc disease is related unless the history is suggestive. If the surgery happened many weeks ago, her pain *might* be managed most appropriately as neuropathic pain. However, I could be wrong. I'd recommend consulting the OB/GYN or a pain specialist if the pain seems unusual (e.g., it persists beyond the usual postop recovery period)...
Hi :)
I came across this article while researching referred pain...there isn't much out there that I could find.
I have a question that I would love if you could answer. For awhile, almost 5 weeks, I've had back pain on my left side right next to my shoulder blade, in between the spine and shoulder blade. It's in a very specific place that I can pinpoint. And it comes and goes with different levels of severity (usually a dull pain that sometimes, not too often, becomes a stabbing pain when I breath in deeply). Occasionaly I have a dull ache in my chest that moves around (left side and sternum)I've also had a cough for the past 9 weeks. The cough hasn't gone away....despite a round of amoxicillin, doxycycline, and 2 rounds, one right after the other, of azithromycin (z-pack). The antibiotics were each about three weeks apart due to respiratory infections. I also had a chest x ray which came back negative.
I was wondering if you could give me your opinion of what this might be and if I should be worried?
Thank you :)
Ashlee
Premed student btw :P
And I just finished anatomy class...I LOVED it!!!
This was awesome but I have one question. If the pain in my sholder is in fact referred pain, would pusing on the spot where I feel the pain make it worse?
I know pain quite well. Wow, 20 years of it. I'm getting old. Dune buggy accident. Cut wide open 3 times and I guess a thoracotomy surgery. There is where my problem lies I believe. Cut from my back, under left arm ending at my breast. Lucky? It's debatable. Post thoracotmy syndrome, intercostal nuerolgia, and symphatetic nerve dystrophy. Obviosly, I can't spell medical terms. I have finally laid down that absolute bottle. Hoping to begin again with the doctors. Some days my hair touching my neck or my clothing being on my back raises my pain level. They used me as a text book in the trauma ICU. I believe if they would have been interested enough to follow through with my "long" recovery they perdicted, they may have been the wiser. My pain doctor told me he would always be there, he would never throw me out in the streets untreated. He lied and I found my medicine at the liquor store. Keep up the studies and I have a feeling you have dreamed the best dream for you.
Great stuff
I am a family Physician from Uganda, East Africa also teaching at the Makerere Medical school. I appreciate this site and your info. Good Luck with Medical School. Consider yourself invited to Uganda for an elective especially on Family Medicine.
Dr Atai
I've had the same shoulder pain for over 10 years and had my gallbladder removed last year, but my pain persists. Now I also have pain in my lower right abdominal area. What is going on?
Ashlee, sorry for the delay - I've been out of town. Part of your description sounds like pleuritic chest pain, i.e., a sharp pain that is aggravated by breathing deeply or coughing. There are many causes of pleuritic pain - such as pneumonia, rib fracture, lung cancer, pneumothorax, pericarditis, and pulmonary embolism - but most of those would show up on a chest x ray. A pulmonary embolism probably *wouldn't* show up on CXR, but seems unlikely unless you have risk factors (e.g., prolonged immobility, cancer, pregnancy, oral contraceptives, hypercoagulable state). I can see why your health care provider gave you antibiotics - in a young, otherwise healthy person with your symptoms and a negative CXR, a respiratory infection seems like a good bet (pneumonia doesn't always show up on CXR). I would also think about gastroesophageal reflux disease (GERD) and maybe pericarditis. See your doctor if things aren't getting better!
Anonymous on 12/23, my understanding is that pushing on that spot would *not* increase the pain if the etiology is referred pain...unless you push really hard!
KHKuhl, hard to say what's going on without more information. Right lower quadrant pain has many possible causes, including appendicitis, gastroenteritis, irritable bowel syndrome, pelvic inflammatory disease, various ovarian conditions, diverticulitis, etc.
Hi. My mother has intense left shoulder pain that has persisted for about 3 weeks now without relief. When she stands or sits it hurts the most and she can't sit or stand for prolong periods of time without lying down for awhile. She's been to the doctor but he didn't examine it and said it was Wry neck . Something I've come to understand that doesn't involve any of her symptoms.
She's had problems with her gallbladder (gallstones) in October 2009 and liver problems a few years back (which was never diagnosed). The pain pills only take the edge off. She wants to know if this pain could be referred pain since she had the referred pain briefly with her first child.
Thanks (this article was very helpful and easy to understand)
i liketheway you explain things mine is a lil different but have been expiriencing pain on my skin and it lasts a day or more but less than a week and my skin hurts to the touch but if i press hard i cant feel the pain but if i brush against my skin or when my clothes touch my skin, here is the problem it affects different parts of my body on different times and it doesnt follow one side of my body it shifts, however i have noticed i experience this after moments of great stress and emotional pain tht i do not express or try to ignore...its not shingles all my gps have failed to diagnose it
Hi :)
I wanted to thank you for your reply! The coughing has stopped. I think it was probably due to stress, but the back pain is still there. I was wondering...could it be caused by a swollen lymph node?
Ashlee
Hi Brad,
Was wondering if you could clarify if my pain I had today was referred pain. Today, about 4 hours after I ate breakfast, my abdomen, especially below the rib cage hurt like no other. It got worse with walking, sitting straight and breathing. Shortly after my ab started to hurt, my R shoulder started to hurt too. This went on for about an hour and since then, I have not had any other probs(nor have I before today). Is this a classic case of referred pain due to my gallbladder? (tis what I was thinking due to my R side below rib cage was the most tender of my ab). Thanks so much for all your help!
Anonymous #1 on 1/14, is her shoulder feeling any better? Based on your limited description, referred pain is one possibility, although it's on the wrong side for gallstones or liver problems, which usually cause pain on the right side. Musculoskeletal problems are much more common causes of shoulder pain than diseases of abdominal organs, so statistically the diagnosis of wry neck seems like a good bet. It's hard to know what's going on without a more detailed history, physical exam, and possibly some imaging or other tests. If you're not satisfied with the current diagnosis, consider following up with the doctor or getting a second opinion.
Anonymous #2 on 1/14, I'm not sure what to make of your symptoms - I haven't learned about any diseases that fit that description. How long have you been experiencing this pattern of pain? Is there an associated rash or other skin changes, or just pain?
Ashlee, I'm glad things are improving a bit. I haven't heard of a swollen lymph node causing back pain, although I suppose it's possible. There are posterior mediastinal nodes that theoretically could grow large enough (e.g., from infiltration by cancer cells) to compress and irritate nerves that innervate the back. That said, I think the other possible causes I mentioned earlier are much more likely.
Erin, your description sounds like referred pain from a gallstone attack (biliary colic), although there are other possibilities. If it *was* a gallstone attack, there is a fairly good chance (about 2/3) it will happen again within a couple years. Risk factors for developing gallstones include obesity, being female, increasing age, and a history of multiple pregancies.
I am starting my third day of fairly acute (7/10) epigastric pain. I have a lot of back issues (which I have successfully ignored for a number of years--high pain threshold!) and had just had a "pain mapping injection" for C3-4 (I have , in which the pain went away 100% but when the Lido/Marcaine wore off (4 hrs or so), the neck felt OK but the upper abdomen--wowee! Nothing helped, I actually started running a low grade fever. Went to the AM PM clinic, had GI cocktail (ew), only fair result if any, WBC's were at 14.6. Sent to the ER. They were concerned about cardiac, hepatic, gastric, cholecystic, pancreatic, even splenic issues. I had another CMP, another CBC, ultrasound, and, thankfully 4mg of morphine + 4 mg of ondansetron IV. (That helped! I've pushed a lot of MS but never received any. It is a good, good drug for pain.) Anyway, I finally got to go home around 3, it was an hour's drive, my gut is already hurting again half way home. I'm thinking (again, and it didn't work last time) I'm just hungry. I ate, it didn't help, but I was seriously exhausted, and finally slept around 5. At 7 I was awakened by the intense pain AGAIN. Went to the kitchen and mixed my own GI cocktail. Worse EW than at the clinic! Didn't help either. Back to bed. Woke around noon convinced I was going figure this out one way or the other and after an hour or two of reading, found this entry in your Anatomy Notes. Thank you. It makes incredible sense. I am going to do a few things now to lower C spine and see if that helps at all with the gut pain. THANK YOU, not only for helping me today, but I am an MSN/FNP student (my heart went pitty pat when I saw "clinical pearls" mentioned on your blog), and I plan to use this to help me become a better diagnostician.
Hi, stumbled across your website. Just a little worried about the shoulder pain that I have now.
I am a 20y/o male, generally healthy - no previous complications.
About 5 days back out of a sudden when I wake up in the morning, I felt this slight pain sensation *inside my left shoulders*. It didnt felt like anything before - the pain is more toward the upper part of the chest rather than close to the heart.. about 4-inches above my left nipple, if that helps.
The pain lasted consistently till now, with no change in intensity. I foudn out actions that worsens the pain. When I take inhale, the pain comes. Exhalation seem ton ot bring the pain. Also, the pain returns after I eat - especially so if it is a large fill.
There is no pain when I am idling - just slight discomfort during normal inhaling. I would test for the pain by taking big inhales.
So far, those are my only symptoms - reading your article conjures thoughts of gastric cancer and some unfortunate scenarios for myself, although I really hope otherwise
Can you please advice/shed light on what is going on here generally?
Regards
Hi Questle,
Obviously I can't give you a diagnosis or medical advice but in someone your age the most likely causes of the pain you're describing (which, similar to a previous reader, sounds like pleuritic chest pain) are musculoskeletal or pulmonary. I'd think about things like costochondritis, pneumonia, and spontaneous pneumothorax, to name a few. It could also end up being idiopathic and self-limiting, in other words, a mysterious problem that goes away on its own. Gastric cancer seems very unlikely because it usually affects the elderly...as always, see your doctor if your condition gets worse or doesn't improve over time.
Many thanks to your response, Brad. Keep up the informative writings!
I had to come back by here and tell you how much you helped me after I had surgery a little over a year ago. I required a distal pancreatectomy, a cholesectomy and a splenectomy due to a 15cm mucinous cystic neoplasm attached to my pancreas.
When I was once again allowed to drink fluids I was hit by horrendous pain in my left shoulder whenever I would swallow. The pain was horrendous! That is the only way I can describe it. Any time I swallowed either liquid or food I was hit with pain like a huge thunderbolt that would actually cause me to lurch or try to leap from the bed (I couldn't move a whole lot). My doctors could offer no answer or help. Although I was still on morphine and it controlled the pain from the surgery, whatever this was, it over-rode the drugs!
I almost felt I wasn't being believed and when I spoke with my physiotherapist a few weeks later she mentioned something to me called 'referred pain'. I googled and found this site and your wise words. They gave me some comfort- here was someone who was talking about pain that sounded similar to mine. So maybe I wasn't imagining the pain. I WAS really feeling it despite the incredulous looks I received from my doctors.
The surgeon did state that both my stomach and diaghram were 'traumatized' during the surgery due to the procedure and the tumour being 'glued' to them as well.
The pain when lasted a good 6 months. What made it bearable? Knowing it would go away in time and it wasn't 'in my head'. Knowledge is power.
Thank-you and enjoy your profession!
Interesting information about Referred pain This theme serves to educate people in their daily life, thanks to people like you we have more knowledge about this important issue.
Brad,
I have been searching for my answer for 6 months, I have never come accross a website as useful as yours.
I am a 44 yr old woman, had upper abdominal pain, it took doctors months to diagnose that I had more than one inch and a half size stones. My gallbladder was removed in September. Couple of weeks prior along with my upper stomach ache I started feeling poking pain on the right side of my left shoulder blade. Two weeks after my surgery I started feeling the same pain and then it traveled to my upper back, between both shoulder blades, then up to my shoulders and neck. My arms started gatting numm too. My doc sent me to orthopedic dr, did xray of cervical, thoratic spines all is normal, he recommended to give a cortizone shot from my spine - I refused. I then thought of referred pain and went to gastro dr, he did MRCP and CT Scan wih contrast. The findings were - dialation of my bile duct 11mm in size, black spot on my liver (per doctor it is highly likely to be a blood vessel). My pain in the upper back is for four months now, between shoulder blades and sometimes severe, although I sleep well at nights but the pain is there daily. Now for the last two months I have been having upper stomach pain, chronic ones. Gastro dr did endoscopy in December 2009 and due to a thick foldon my stomach a biopsy result came as inflammation and he prescribed me Nexium. Stomach pain is there but not every day. No hearburn, no bloating, although a lot of gas. They can not find the answer, now the dr recommends doing EUS or ERCP to check why my bile duct is dialated as it is 10mm per dr norm should be 5mm for my age. Just to mention the doctor is very respected in the hospital and does not think my upper back has any relation with my organs, as he thinks it is all musculatory pain as I have worked 25 yers mainly in front of the computer and a very stressful job n IT. The doctor did leave the option of having EUS to me if I agree. As I am sitting now and typing this hoping to have some answer from you and some suggestion or advise. My pain is constant in the upper back. To mention one interesting fact, when upper stomach hurts, upper back does not, when stomach pain stops upper back then starts hurting. I agreed for EUS but not sure for ERCP. Most likely will be scheduled in couple of weeks. Thank you so much in advance. Your feedback will be hugely appreciated as I am sufferrng for 4 months with no results....
Worried and Hopeless,
Sounds like your case is very challenging, both for you personally and for the doctors who are trying to sort things out. The key question seems to be whether the pain in you back is referred pain from your abdomen (stomach? bile ducts?) or musculoskeletal pain. The pain you describe doesn't fit clearly into either category; in fact, it could be both. Perhaps an initial episode of referred pain triggered a back spasm that led to pinched nerves and arm numbness. If the pain is primarily due to muscle spasm, you'd expect some relief with exercise, physical therapy, and ibuprofen. I can see why your doctor would want to do EUS or ERCP to rule out an ongoing problem in your biliary tree. However, you may want to clarify what he is looking for, since your abdomen has already been imaged extensively. What could he find with EUS or ERCP that wouldn't show up on MRCP or CT? I'd also be interested to know if anything in your physical exam or labs shows evidence of biliary obstruction (http://emedicine.medscape.com/article/187001-overview). I wish there were an easy answer....keep me posted!
what about the symptoms for women and heart problems? isn't it true that women may have very different referred pain symptoms...not hte usual left arm/shoulder pain?
It's true that heart attacks in women can feel different from heart attacks in men, adding to the challenge of accurate diagnosis. Check out this link for more info:
http://www.medicinenet.com/heart_attack/page7.htm#diagnose
As far as I know, no one knows why these differences exist.
I just learned about referred pain...my Dad (90 years old) was recently diagnosed with mesothelioma and had a pleural catheter inserted to drain fluid accumulating around his left lung. Immediately following his first full drain he experienced SEVERE pain in his left shoulder. So intense I thought he was having a heart attack. We chalked it up to a muscle spasm. The second drain was a partial drain and he experienced no pain. The third drain was a total drain and the pain returned right at the end of the drain. So intense he was writhing on the bed. After reading the information of referred pain it is so obvious the pain is referred from his lung area.
Brad,
I am responding from our last conversaton on 02/11/10.
I had my EUS and ERCP last night and the result was narrowing of bile duct, therefore the doctor dialated my bile duct, pancreas and the rest was normal with no complications. I am releived and happy that there were no complications or sad surprises. I have no stomach pain for almost two weeks. Unfortunately my pain between my shoulder blades is still killing me daily. I am going to physical therapy as well as a chiropractor, the pain is since September 2009. Please advise what/which area of my body should I have examined, rulled out to help doctors narrow the search and hoping find the cause of my pain. I am in pain every day and the pain is mainly around my choulder blades and sometimes on the spine as well. Have had cervical mri all came normal. I am hoping it is nothing serious therefore am trying to search the body parts to be tested to rule out any dangers.
Please advise and Thanks again,
Worried and Hopeless....
Worried and Hopeless, my impression is that you've undergone all the standard tests to rule out life-threatening conditions. If chiropractic and/or physical therapy are helping at all, I would continue them and add cardiovascular exercise and perhaps stress reduction exercises if you haven't already. Painkillers can also have some benefit although they come with their own risks (as I'm sure you know). I wish I had more ideas....
Thank you Brad. Which professional you think would be best for my situation orthopedic or neurologist? Thaks again for your time.
Worried and Hopeless
At this point a neurologist might be more helpful, especially if they have experience with pain management. Another option to consider is a pain clinic where they can do interventional pain procedures like facet and medial branch blocks. Here's a nice FAQ:
http://www.brighamandwomens.org/anesthesiology/Pain/Patients/blocks1.aspx?subID=submenu3
I have read your blog more than once and have found it to be very interesting and useful.I am a 28 year old female and I myself have had back pain for awhile now. I first started feeling the pain about a year ago. The pain was mostly felt in the right shoulder area and middle right back. I seen my family doctor for this problem and he suggested physical therapy. I did not follow through with the physical therapy because the pain had went away.(I never really felt that the pain was just typical back pain) Now the pain is back and I feel it sometimes just in the right shoulder area and sometimes just in the middle right back.The pain is dull and persistant but does not affect my day to day life. I also have noticed pain/burning sensation under my rib cage. Could the pain I am feeling in my back be related to my pain in my upper stomach?Is the pain I am feeling referred pain and is something that I should be worried about? I would greatly appreciate any info/advace that you may have.
I would suggest for you to see your family physician again and ask him if it could be stomach acid, inflamation some sort of, or it could also be due to your muscles,personally do not beleive in Physical therapy for every pain. Your body knows if the pain is a muscle pain. If you feel it is not helpings, then do not waste money, work closely with your doctor to rule out any organs (refferred pain). Hope this helps. Please let me know the outcome.
Good lUCK
28 yo female, I agree with the above post. Your back pain could indeed be referred pain related to a problem in your gall bladder, stomach, etc. Talk to your doc again and express your concerns.
Brad,
I have been scheduled for epidural shots on my neck for upper back pains.
My upper stomach chronic pain every other week or so is still there. It is more on the upper stomach and comes 4 days in a row and them no pain for 10 days, then it comes again. I have a lot of gas as well in between the days. I can eat any food it does not bother or hurt, not heartburn or nausea. The pain seems has its own schedule comes and goes regardles. I had the EUS and ERCP and all came normal. Have gallbladder removed last year. What could be the possible cause?
Thanks as always.
Hopeless and Worried
Hopeless and Worried, unfortunately there are many causes of abdominal pain, and not all of them show up on lab tests or imaging studies. One very common example is functional dyspepsia:
http://www.utdol.com/patients/content/topic.do?topicKey=~ATpoXQDeq.jDgA
Does the description at that link seem like a good fit?
Brad
Thank you for the link. By reading the symptoms it is very similar to mine. I do have a follow up appt next week with the doctor that did my EUS and ERCP. Will keep you posted of the diagnoses.
Thanks for your time.
Worried and Hopeless.
About the best blog I've found in a long time, the only one I've wanted to leave a comment at. I found omitting gluten from my diet freed me instantly of GERD I'd fought with H2 blockers and Gaviscon for a long time. Now I have a question that's stumped the doc's I've seen. Had an epidural this morning; the anestheologist who performed it did not think it would do what the neurologist did who ordered it.
Tingling about the size of a large dinner plate from just below my waist line up, started 6/6/06, evening when laying down, like someone flipped a light switch, most noticeable when laying down, never any change in intensity, no pain. Intense enough that I take Ambien 5 when I am not working 12 hour nights so that I can sleep. I am 67 years old, have bundles of energy, had breast cancer 11 years ago and again a year ago. I say I am a member of the empty cups runneth over club. Any ideas? Thanks for such an informative blog. You are going to be a GREAT doctor! Lucky for your patients!
Hi Nightnurse, My apologies for not responding sooner - it's been a busy time with Match Day on the 18th (i.e., the day I find out where I'm going for residency). Anyway, let me make sure I understand your story. You've experienced persistent tingling that started suddenly almost 4 years ago. Beyond that I'm not sure I have a clear picture. Where exactly is the dinner-plate sized patch of tingling? Centered on the midline or off to one side? The tingling doesn't change in intensity, yet you notice it more when you're lying down - could you clarify that? Is there any numbness or other associated symptoms? Does anything exacerbate it or relieve it? And why did you get the epidural? So far I don't have any good ideas...
Hi ! thanks for your blog! I see lots of questions on the internet (never answered)about the same pain as me. That is a tight pressure feeling in my left upper arm just like a too tight BP cuff. I just learned from some of my friends,that they had the same thing diagnosed as referred pain from a gastric ulcer.
WOW - I had that on and off for ten years and when I had a gastroscopy for another reason, they found a gastric ulcer. Why is this missed in so many people? I've had 2 complete cardiac work-ups at considerable cost telling me my heart is OK and my arm pain must be something wrong with my shoulder. Have you heard about this type of pain in an ulcer?
I *have* heard about referred pain from a gastric ulcer, but my impression is that it's uncommon, which could explain why others have missed it...
Hi..This blog is heaven sent. I have been searching for a cause of my constant lower back pain and RUQ pain. Had every test known to man. The lower back pain presented first. I've been on a heating at night for several years..but then the pain just beneath the right rib and right upper stomach area started. Am I correct in thinking that my lower back pain above sacrum center and right may be caused by my gall bladder? I have yet to do the Hida Scan (a bit chicken) and the pain is now constant for 18 months. The only thing the scans showed was an hemangioma which they tell me cannot cause my pain. The doctors say in no way are the lower back pain and gallbladder related! I'm confused and in miserable mmost of the time. Any ideas?
Back pain and abdominal pain can be among the most vexing diagnostic challenges in medicine - in many cases no definitive cause is ever identified. Could your gall bladder be the source of your back pain? It seems unlikely, but it's hard to be certain. If your doctor recommends the HIDA scan, I'd probably do it (after resolving your concerns with a doctor or getting a second opinion) - it may be your best chance to rule out gall bladder disease. Keep us posted...
Hi Brad...
Thanks for getting back to me so quickly. I am going to do the Hida Scan. I did read on a number of other posts from people with gall bladder issues, that they had low back pain. However, I don't know how low...maybe just beneath ribcage. I do know in oriental medicine where the gall bladder meredian runs along the body and some oriental medicine websites say that even knee pain (popliteus muscle to be exact) can be affected due to gall bladder and cause a weakening of the knee joint thus creating instability and pain. Don't know how reliable that is. It just seems strange that my left knee has Baker's Cyst now and swells frequently. I just know the RUQ pain is constant dull ache and I have other gall bladder symptoms as well. It's all very interesting albeit frustrating when it's you with the pain! Do you believe there is any merit to the oriental meredian theory? Thanks.
Bufalowgrl, I look forward to hearing the results of your HIDA scan. I haven't heard of an association between gall bladder disease and weakening of the knee joint (or a Baker's cyst)...seems unlikely, but who knows. I don't know much about meridians, but according to one physician-scientist, meridians are often located between muscles, where connective tissue planes converge: http://www.uvm.edu/~uvmpr/?Page=article.php&id=2208
Ive had pain in my left shoulder for the past 16 years. My doc said I have fibromyalgia. My pain is so severe, I am on the fentanyl patch, and am still in pain! Can I have the nerve deadened? I wish I could rip my entire are of shoulder off! it is the flat part of shoulder before it hits the neck. It started as soon as I woke up from csection and never stopped.
Dear Brad
This is most informative. Thank you so much for the free information. It has helped to diagnose what is going on with my sister. She was previously obese and had her stomach banded 2 years ago. Up until a year ago she was able to eat normally although not in large amounts. Now protein dense foods such as beef sit in her stomach and cause her referred pain between the shoulder blades. She ends up vomiting the food after an hour or so as she can't take the pain (not that she has ever had a high threshold). At least this aspect of her problem has been highlighted through this article. Sequoia1968
Hi All
I have recently had a laparoscopy to explore right sided ovarian pain I get every month from the start of my ovulation cycle until about the 2nd day of my period.
I have a history of polycystic ovarian syndrome and an ultrasound prior to my surgery confirmed cysts on the left ovary.
My Gyn thought that I may have adhesions on my right ovary causing the pain.
Instead of this, my doctor found the right ovary in "perfect" condition and the left in a mess. Endometriosis has fused the left ovary to my bowel. The doctor has freed as much tissue as he is able however, further surgery will need to be conducted by a bowel surgeon.
The doctor believes my right sided pain which can be described as a dull ache as referred pain but almost unbearable at times. It hits my right sciatic nerve and travels halfway down my thigh. I have had this pain for about four years.
Unfortunately, 9 days after the surgery I began to ovulate and the right sided pain returned only much, much more painful.
I haven't seen the doctor yet but I think this confirms that it is referred pain as the doctor did not touch the right ovary.
Thanks for this great site, it is comforting to hear of others with similar experiences.
Terri
Perth, Western Australia
Brad, re my entry 3/17 tingling in my back, answering your questions. The lowest edge of the area of tingling lies about an inch below my waist at the midline up to the middle of my shoulder blades and out towards the sides, as if you'd placed a large dinner plate against my back with the rim just below the belt line. I say tingling for lack of a better term. It's like when you put your hand on the casing of a well-tuned motor and you feel the hum, the vibration, of the motor. I can't put my hand on my abdomen or back and feel it; it's deep inside. At times I feel there is something there that moved in on that night in June 206 that has a life of its own. Tonight it's almost throbbing. There's no numbness, no pain with movement. I went to see a neurologist who had advertized a forum he was giving entitled "Do you want to feel like you used to feel?" He ordered an MRI of the lumbar spine; it showed some compression of L3 and L4, thought the epidural might permanently solve this problem. No luck. He prescribed neurontin; he was disappointed it only helped the neuropathy I suffer in my feet due to chemo x 2 for the breast cancers I had. It did nothing for the tingling. Too much salt in the diet or Sudafed can temporarily make the tingling/vibration feeling more noticable, make it feel like it's radiated out towards the shoulders and the base of the neck. I do not have headaches. The massage therapist, physical therapist, chiropractors have all been stumped at why I feel this way... they do not look at me as tho I am crazy when I describe this to them. When I finally shared this with my physician a couple of years ago, I told her that I would not be in her office if everything was all right, I was only there because something was wrong and to please not pat me on the head and send me on my way... she had no comprehension of what I was saying... she had me bending every which way, leaning over, couldn't understand that this is totally within and just because she can't feel it with her physical exam doesn't mean it's not there. As a nurse I have seen patients who kenw for certain that something was wrong and eventually the cause was found but those patients put up with physicians not believing them for a long time and suffering discomfort and distress as well. Do you have any ideas? I hope these blogs will help you in your practice of medicine and I sincerely appreciate your time and interest. God bless you for the help and hope you've already given others.
Fascinating page. Congratulations. I wonder if you can help. I had a colonoscopy (after a CT scan suggested uncomplicated diverticular disease and incidentally a renal cyst) three days ago. I was sedated and watched it. No nasties, but confirmed the CT. Since then, much discomfort from a sensation like having 2 canon balls shoved up behind my ribs from above my stomach. Saw a doctor who listened to colon, said no gassy activity. But the pressure is scary, whether lying, sitting or standing. Could this be referred? My other doctor suspects perhaps an auto-immune pancreas problem because of stomach symptoms. Put me on a proton-pump inhibitor a few days back. Any ideas about the discomfort as it makes me feel quite desperate to tear out the canon balls.
Nightnurse, thank you for the additional information. Yours is indeed a puzzling case - I wish I had a good answer. My best guess is that your paresthesia (the odd sensation you describe in your back) is related to your lumbar compression fractures. Compression fractures can definitely cause pain; maybe they could cause paresthesias too. I don't know how significant your fractures are, but maybe you'd be a candidate for a minimally invasive procedure like vertebroplasty (http://www.radiologyinfo.org/en/info.cfm?pg=vertebro).
Rose107, hard to say if it's referred pain or just plain old visceral pain related to the colonoscopy (e.g., from distention). I'm guessing it will go away on its own, but you should monitor it and talk to your doctor if it's getting worse or not getting better. Get well soon!
Hi I'm a 52 yr old male, for the past 6 weeks or so I have had this pain on my left side lower back which is in my pelvic / hip area, the pain is a dull but burning kind, its pretty painful all the same, its getting slowly worse, any ideas ? I am also more tired than usual..
Hi I'm a 52 yr old male, for the past 6 weeks or so I have had this pain on my left side lower back which is in my pelvic / hip area, the pain is a dull but burning kind, its pretty painful all the same, its getting slowly worse, any ideas ? I am also more tired than usual..
sorry but I dont know how to add my email address on here so if you can help me then please let me know via my email, thank you for your help
tez160@hotmail.com
Hey Brad what an inspiring site- it sounds like you have a very interesting and busy life- I am an MD in New Zealand and know all about doing residency with kids! Good luck and keep writing :-)
I have tooth ache,pressure, on upper left 2nd molar. Dentist took X-rays of lower left 2nd molar and determined that it is infected. It had a root canal done a long time ago. But there is no pain coming from lower molar at all. Is it possible for a problem tooth on lower molar to cause no pain at all...and have referred pain on upper molar?
Thanks, Brad, but the discomfort from the 'canon balls' under my ribs is still around, three weeks later. It's less painful than the pressure feeling I described. But, the whole of my rib cage at the front (I can't reach the back, of course) is painful to the touch. The collar bone no. And there's another set of symptoms. I am getting funny turns, sometimes two or more a day. This happened today, less than an hour ago. Had one yesterday when out in the garden. This time I was inside with my laptop, reading your blog! Feeling faint, sick, feet tingling, singing in ears, head feels detached, slight headache, pains in lower abdomen. Hard to breathe. Tingling moving up from feet. Pain in top of abdomen. Throbbing everywhere. Singing getting louder in ears. Feeling faint. Salivating. 137/69, pulse 66. Feeling very hot. Pains in upper legs, ankles, eyes. Pain over top of head. Hurts to breath in deeply. Trying to get oxygen into lungs. Singing in ears still loud. Very hot. Thanks. Keep up the good work.
23 years ago I was sent to a Physical therapist for constant pain in between my shoulder blades...after about 15 minutes, he brought out this ancient book, and showed me where the pain I was experiencing was a referred pain, due to intestinal issues. After getting down to 94 pounds, 8 days in the hospital, I was diagnosed with Crohn's Disease. I still experience the abnormal referred pains, which is one of the first indicators that I'm getting ready for a bad flare-up. It's still weird though!
Cena, I haven't heard of referred pain from the lower jaw to the upper jaw, but from a neuroanatomical perspective it seems possible to me.
Gwynf, I don't have an explanation for your new constellation of symptoms, but most of them (feeling faint and hot, tingling, headache, tinnitus, shortness of breath, salivation, abdominal pain) are consistent with vasovagal episodes (called vasovagal syncope if you actually faint). Vasovagal reactions can have many triggers - such as hot weather, prolonged standing, lack of food, emotion, head movement - or no apparent trigger at all. Again, if you're concerned or things seem to be getting worse, talk to your doctor!
Anonymous, thanks for sharing your story. I hadn't heard of referred pain from Crohn's, but it makes sense!
Re the symptoms, doctor now thinks it might be abdominal epilepsy after a severe blow to the left forehead after a fall two years ago. That's when it all started. Thought that might help someone.
Hi Brad,
I have been trying to find a website like this for quite some time! I had my gallbladder removed two weeks ago because I had biliary dyskinesia which led to an infection. While trying to find the problem, I had upper back pain every few weeks that was not in the normal areas for referred pain for the gallbladder. I thought that having it removed would also get rid of the problem. My doctor didn't really know how to help me out, actually, he didn't really try. It started out with pain right in between my shoulder blades, but to the left of my spine. It feels like somebody is taking a screwdriver and stabbing me. This is the same spot that the diagram shows referred stomach pain; however, four months ago I had an endoscopy with normal results. Other times, the pain in my back is a thick strip parallel to my stomach. It causes me to wake up at night and occasionally eating relieves the pain. The pain also usually only occurs in the evenings. Do you have any suggestions? Could my gallbladder (or lack of it) cause this pain, could it be my stomach, or another unknown source? I would appreciate any insight.
Thanks,
Andrea
Andrea, without seeing you and having access to your medical history, test results, etc., I obviously can't make a diagnosis; however, I can share a few initial thoughts. Back pain has many causes, but I agree that yours sounds like referred pain, possibly from the GI tract given that the pain is occasionally relieved with eating. In spite of your negative endoscopy, a duodenal ulcer would still be high on my list. I would also wonder about chronic pancreatitis and maybe a kidney stone, and I would want to rule out serious disorders like cancer, acute coronary syndrome, and aortic dissection (although these things are unlikely if you're a young nonsmoker). I'm also curious if the nature of the pain changed at all after the cholecystectomy. If it did, maybe the pain *was* related to the gall bladder and now you're experiencing post-op pain that will hopefully dissipate with time. As always, your best bet is to see your doctor (or another one if the first one isn't helpful).
G'day from the Land DownUnder, I have a 2.5cm cyst with vascularity and septa on my left ovary, which was found on ultrasound. Went for the US as I was having RLQ pain intermittently. Had the usual CT, ultrasound, etc all normal on the RLQ. My question is; is it possible that the pain on RLQ is actually referred from the left? My doc when I put it to her said, I guess anything is possible.
Just curious as to your thoughts.
Great blog by the way!
Cheers!
Hi Ria, RLQ pain referred from the left ovary would seem unlikely, but it turns out that someone else from Australia described something very similar about a month ago (Terri from Perth on 5/12/10). Her story appears to be a surgically confirmed case of referred pain from the contralateral ovary. Interesting, isn't it?
Brad
Thanks Brad! I must have zoomed through all the posts too fast and missed that one! I have read her post and yes, it is intriguing! Must be an Aussie thing with ovaries! Ha ha!
Hope you are doing well in your 'rounds' I look forward to reading more in your blogs!
Cheers!
Thanks Brad! I must have zoomed through all the posts too fast and missed that one! I have read her post and yes, it is intriguing! Must be an Aussie thing with ovaries! Ha ha!
Hope you are doing well in your 'rounds' I look forward to reading more in your blogs!
Hi I'm May and I wanted to ask you something about a pain that I originally experienced in my left shoulder a couple of months ago (march) and it was accompanied by a high blood pressure of 190/100. I had it checked up and I was given a prescription for my hypertension and high cholesterol. Two medications for hypertension and one for the cholesterol as part of my maintenance. For a month my medication was reduced to a single hypertensive drug due to a positive outcome, my BP was normal. Nothing was explained about my shoulder pain except that it was a "frozen shoulder". I was unable to raise my arm and the pain didn't really go away and endured it until I got used to it. I just performed a couple of stretching in the morning and the usual workload for my arm. And now, I again experienced the pain but it involves my right shoulder. From the onset of the pain it radiated to the back of my head and it was again accompanied by a high blood pressure of 200/100 and a little amount of pain in my chest. It has been for three days that I am enduring my pain. I can't raise my arm, It is so painful all throughout the day, and it is unrelieved by an ibuprofen. My BP now is normal because I am again taking 2 hypertensive drugs but my shoulder really just hurts a lot. What am I experiencing? Am I having a TIA? MI? Angina perhaps? What laboratory or diagnostic procedures should I undergo to know what is exactly happening to me?
I'm looking forward for your answers and thanks..
Hi Anonymous, sorry for the slow response - first week of intern year has been crazy busy (as expected). Most (95%) cases of high blood pressure are garden-variety "essential" hypertension, i.e., the kind that tends to show up in middle age, run in the family, and be associated with things like obesity, sedentary lifestyle, and high-salt diet.
However, in some cases, there is an underlying disease that may be treatable with something besides blood pressure meds. We think about these unusual causes of hypertension if it shows up suddenly, especially in patients less than 20 years old or greater than 50, or if the blood pressure is very high or resistant to treatment with blood pressure meds.
I don't know your age or other key elements of your history, but your description of sudden-onset episodes of very high blood pressure accompanied by chest pain and headache do make me wonder about rare secondary causes of hypertension such as pheochromocytoma. I don't have a good explanation for the shoulder pain - it may or may not be related...
Part 1 of 4 (only I hope)
What a beautifully lucid account of referred pain I found when I started Googling for which I shall come back to. Now I want to put the immediate cause of my interest in my body's pains as a question about a hypothetical cause of the back pain which caused me to forfeit a Real Tennis (aka Court Tennis in the US and Jeu de Paume in France) match this morning in Melbourne, Australia. So, to my brief first question/proposition
1. As I have managed the consequences of old age and a twice prolapsed L5/S1 disk for over five years by a few minutes of stretching warm up (including back stretches by one leg over the other and back arching from a prone position) before I play I am surprised that, in the last three weeks I have had spasms across my lower back which require careful straightening out of my back, and quite a bit of warming up before I can do anything demanding - though the demanding tasks have included an hour's singles. Could it be because someone taught me a few weeks ago that the essence of improving core strength was to tighten and pull in hard the muscles between the pelvic bones and, as a result I decided to add that form of exercise on an irregular basis but quite frequently a three or four weeks ago? The match I played today and had to forfeit after playing for about 50 minutes when the second attack of back spasm proved too severe to dissipate quickly was against a medical doctor who acknowledged that I wasn't talking nonsense in hypothesising that I had upset some existing balance by my core muscle contractions.
Part 2 of 4
2. My other question/proposition is about a pain in the hip (can be either, not as far as I can remember both at the same time) when lying flat on my back in bed. I can ease it by putting the associated leg over the edge of the bed and/or by stretching my whole body from feet (sometimes with toes vertical sometimes pointing away from my trunk) to head so that, presumably because that is what it feels like and is what I intend, my back is stretched though not as thoroughly as on an inversion table. What is that all about? Here follows the background:
I am 72, 184 cm, 81 kg (though down to 76 kg before Real Tennis competition in New York in 2008). I try to play 2 x 1 hour singles and 2 x 2 hour doubles each week and use the warm up on court to go straight to the club gym for 20 minutes of heavy resistance exercises.
10 years ago I had a prolapse of L5/S1 from which I recovered almost completely but in late 2004 I had another which, after three months of dealing with pain and exercising only by swimming left me with numbness of the right foot and slightly weakened right lower leg. Since then I have maintained leg strength in the gym and can scuttle around the court quite fast but my left foot has also been slightly numb for a couple of years. I take that not to be what you would call a "referred" effect or pain but a result of direct pressure on the sciatic nerve.
I have an inversion table that I used for a few months on my own hypothesis that I might give my L5/S1 area a chance to fix itsef with an intermittently improved blood supply but, like most people, gave up.
Part 3 of 3 (not 4 as supposed above)
One last clue as to my occasionally hurting hips. After racing on to the lawn tennis court on a winter day in 1982 without warming up I damaged some muscle fibres in my left lower back and, after dealing with the next few days pain by ineffectual hot baths and more useful tranquillisers or Valium or some such I was left with no more residual problem but a tendency for my left hip to hurt after various events which made me associate the pain with the 1982 back injury. One experience was that of loosening up my back muscles by sitting for a long time - typically in a long distance aircraft - and then having to stand at a cocktail party or in an art gallery. The pain in my left hip was quite reliably there. I also felt compelled to give up the jogging I used to do (to the point where I had rund a marathon in 1979) and did quite a bit of experimenting with insoles for my everyday shoes as well as looking for better cushioning in sports shoes (now happily standard but I read somewhere that one ought to go back to effectually barefoot running with just a skin of protection for one's soles - that's just BTW for present purposes I think).
So, would it be right to suppose that my earlier left hip problem was the result of a nerve from about L4 or above suffering damage from my 1982 mishap but that my lying flat in bed problem for both hips is probably an L4 or above compression which, apart from the easing by stretching that I have described I can do nothing much about?
Part 2 of 3 (was 4 but not needed) - apparently I can only post once a day
2. My other question/proposition is about a pain in the hip (can be either, not as far as I can remember both at the same time) when lying flat on my back in bed. I can ease it by putting the associated leg over the edge of the bed and/or by stretching my whole body from feet (sometimes with toes vertical sometimes pointing away from my trunk) to head so that, presumably because that is what it feels like and is what I intend, my back is stretched though not as thoroughly as on an inversion table. What is that all about? Here follows the background:
I am 72, 184 cm, 81 kg (though down to 76 kg before Real Tennis competition in New York in 2008). I try to play 2 x 1 hour singles and 2 x 2 hour doubles each week and use the warm up on court to go straight to the club gym for 20 minutes of heavy resistance exercises.
10 years ago I had a prolapse of L5/S1 from which I recovered almost completely but in late 2004 I had another which, after three months of dealing with pain and exercising only by swimming left me with numbness of the right foot and slightly weakened right lower leg. Since then I have maintained leg strength in the gym and can scuttle around the court quite fast but my left foot has also been slightly numb for a couple of years. I take that not to be what you would call a "referred" effect or pain but a result of direct pressure on the sciatic nerve.
I have an inversion table that I used for a few months on my own hypothesis that I might give my L5/S1 area a chance to fix itsef with an intermittently improved blood supply but, like most people, gave up.
I have tooth ache,pressure, on upper left 2nd molar. Dentist took X-rays of lower left 2nd molar and determined that it is infected. It had a root canal done a long time ago. But there is no pain coming from lower molar at all. Is it possible for a problem tooth on lower molar to cause no pain at all...and have referred pain on upper molar?
Post a Comment
<< Home