
Referred pain
Updated July 2009
If you woke up with a pain in your shoulder, you'd probably think something was wrong with your shoulder, right? Maybe you slept on it the wrong way, maybe you're a weekend warrior who threw the football a few too many times. In most cases, your hunch is probably right. Pain in the shoulder usually indicates an injury or disease that affects a structure in your shoulder, such as, say, your subacromial bursa or a rotator cuff tendon. Makes sense, doesn't it?
But you might be way off. Sometimes the brain gets confused, making you think that one part of the body hurts, when in fact another part of the body, far removed from the pain, is the real source of trouble. This curious (and clinically important) phenomenon is known as referred pain. For example, it's unlikely but possible that your shoulder pain is a sign of something insidious happening in your liver, gall bladder, stomach, spleen, lungs, or pericardial sac (the connective tissue bag containing the heart). Strange, isn't it? Conditions as diverse as liver abscesses, gallstones, gastric ulcers, splenic rupture, pneumonia, and pericarditis can all cause shoulder pain. How is that possible?
Neuroscientists still don't know precisely which anatomical connections are responsible for referred pain, but the prevailing explanation seems to work pretty well. In a nutshell, referred pain happens when nerve fibers from regions of high sensory input (such as the skin) and nerve fibers from regions of normally low sensory input (such as the internal organs) happen to converge on the same levels of the spinal cord. The best known example is pain experienced during a heart attack. Nerves from damaged heart tissue convey pain signals to spinal cord levels T1-T4 on the left side, which happen to be the same levels that receive sensation from the left side of the chest and part of the left arm. The brain isn't used to receiving such strong signals from the heart, so it interprets them as pain in the chest and left arm.
So what about that shoulder pain? All of organs listed above bump up against the diaphragm, the thin, dome-shaped muscle that moves up and down with every breath. The diaphragm is innervated by two phrenic nerves (left and right), which emerge from spinal cord levels C3, C4, and C5 (medical students remember these spinal cord levels using the mnemonic, "C3, 4, 5 keeps the diaphragm alive"). The phrenic nerves carry both motor and sensory impulses, so they make the diaphragm move and they convey sensation from the diaphragm to the central nervous system.
Most of the time there isn't any sensation to convey from the diaphragm, at least at the conscious level. But if a nearby organ gets sick, it may irritate the diaphragm, and the sensory fibers of one of the phrenic nerves are flooded with pain signals that travel to the spinal cord (at C3-C5). It turns out that C3 and C4 don't just keep the diaphragm alive; neurons at these two spinal cord levels also receive sensation from the shoulders (via the supraclavicular nerves). So when pain neurons at C3 and C4 sound the alarm, the brain assumes (quite reasonably) that the shoulder is to blame. Usually that's a good assumption, but sometimes it's wrong.
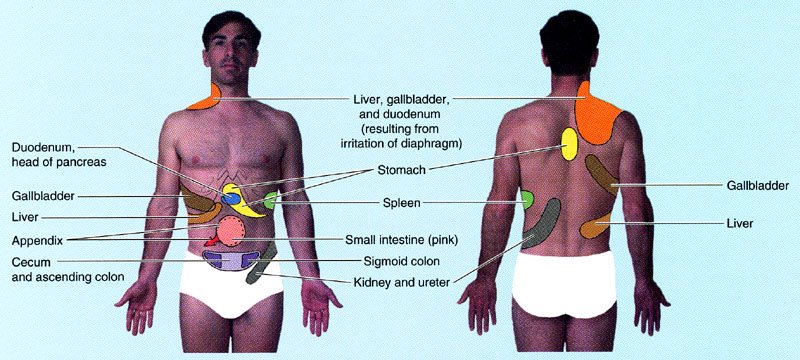 Illustration showing sites of referred pain from abdominal organs. From Moore and Dalley's Clinically Oriented Anatomy. Please note that I added the "tighty whities" with Photoshop (hey, this is a family friendly site).
Illustration showing sites of referred pain from abdominal organs. From Moore and Dalley's Clinically Oriented Anatomy. Please note that I added the "tighty whities" with Photoshop (hey, this is a family friendly site).Another example that seems bizarre until you know the anatomy is disease in the stomach causing pain between the shoulder blades. A classmate told me that one of her college professors complained to his doctor about pain in his upper back that wouldn't go away. It turns out that the professor had gastric cancer, a relatively aggressive and often incurable disease unless it's caught early. Unfortunately it wasn't caught early enough and it ended up taking his life. Maybe the outcome would have been different if the doctor had remembered that some of the nerve fibers to the stomach (specifically, visceral afferents that travel in the greater splanchnic nerve) convey pain signals to the same spinal cord levels (especially T5 and T6) that receive pain signals from the skin between the shoulder blades. This variety of referred pain is rare, but it happens often enough to be mentioned in anatomy textbooks.
Not all cases of referred pain are easy to find in textbooks. Take the appendix, for instance. That wormy little appendage of the colon is usually located in the right lower quadrant of the belly, nowhere near the diaphragm. Typically people with appendicitis feel diffuse pain or discomfort around the belly button, or sharp pain in the right lower quadrant if the appendix is getting ready to burst. But occasionally the pain refers to the right shoulder. Why? Note that I said the appendix is usually located in right lower quadrant. Sometimes, early in embryological development, the colon doesn't rotate as much as it should, and the appendix ends up in the right upper quadrant (or even on the left side of the belly). That malrotation isn't necessarily a problem for the patient until the appendix becomes swollen with infection, irritating both the diaphragm and the doctor who is trying to make a diagnosis!
So if your shoulder happens to hurt right now, should you be worrying about something bad in your belly? Probably not. The most common causes of shoulder pain are, by far, musculoskeletal problems like osteoarthritis, adhesive capsulitis, and rotator cuff tendinitis. Often, with the help of taking it easy and a few rounds of ibuprofen, the pain goes away on its own. But if you're still concerned, make an appointment with your family physician. Red flags include more ominous symptoms like fever, unexplained weight loss, and pain in the left shoulder or scapular area that gets worse with exertion.
Your doctor will want to know all about the pain. Was there a specific injury or did the pain come on slowly? Does the pain occur without movement of the shoulder? Can you make it worse with specific movements? Are there any other symptoms or chronic medical problems? The answers to these questions, along with a physical exam and appropriate imaging studies, will provide the information your doctor needs to understand the problem and create a treatment plan. The odds are good that the problem is relatively common and treatable. But if your doctor seems stumped, it wouldn't hurt to ask, "Is there any chance this could be referred pain?"
posted by Brad @ 4:45 AM
338 comments
![]()
![]()


